
By 2025 FDC Speaker Ankur Gupta, DDS
I have seen enough continuing education (CE) courses, given by enough talented practitioners, highlighting the effectiveness of harvesting blocks of bone from the ramus or the hip to come to the following conclusion:
I, a general dentist, will never harvest bone from the ramus or the hip.
I am not saying that it isn’t effective. It certainly is. What I am saying is that I am way too much of a weenie to ever do such a surgery. I’m not even sure how that conversation would go … “before I pull your tooth, could you push your pants down just a smidge?”
So, in my 20+ year bone grafting CE course journey, I have learned all about the keywords cortical, allograft, mineralized, demineralized, bovine, membrane, collagen, etc. This has led me to the following conclusion:
When I pull a tooth, what is the easiest thing that I can shove into the socket where I can predictably and successfully place an implant six months later?
My journey began with the gold standard: bony particulate, with a non-resorbable membrane to prevent gingival penetration into the particulate graft. Ok, sounds easy enough until I finally started stitching. Then, inexplicably, as my silk suture would pass through the surgical site, the membrane would start moving. My assistant would hold it into place with an instrument, causing it to bend and crease. By the time I was done suturing, it would look like a crumpled-up piece of paper was shoved into the socket.

Weirdly, a few months later, the area would actually look ok, but this never made me feel like a great dentist.
Next, I learned about the magic of PRF, PRP and PPP. The idea of converting bony particulate into a packable gel-like consistency sounded amazing, and creating a PRF tissue plug was icing on the cake. Because of the ‘gum-like’ consistency of the PRF plug, I was able to suture over the socket with a much greater level of predictability and control. Actually, I felt like a medium to above-average dentist. The area would look amazing only a few weeks later, and often, the bony particulate would integrate extremely well within the socket. Six months later, I was ready to place a beautiful implant surrounded by a galaxy of healthy bones.
The problem? Well, there are two. First, utilizing PRF and PRP requires the acquisition of a centrifuge. Not only is this an investment, but it takes up space. It also requires a completely new set of ‘phlebotomy’ inventory. Second, unless your training was significantly different than mine, we didn’t receive incredibly extensive phlebotomy experience as general dentists. I tried to “get a vein” about four times during my GPR 20+ years ago, and I’m not sure I was ever successful. Sticking a needle in a person’s oral vestibule is something that all of us have some confidence in, but sticking one into a person’s arm is a different story. Using PRF is great, but unless the patient has a bulging juicy Avenger vein, I feel the nervousness rise as I stare at my patient’s arm.
So, that leaves us with what? Ramus slicing, which is too scary. Membrane placement, which is too crumply. PRF, which is too centrifuge-ey.
Introducing: Plugs
When I was a teenager and begged my parents to allow me to see Aerosmith live concert, they finally capitulated, but only on the condition that I would wear earplugs. You can imagine how cool I looked.
Now imagine the same thing: something that looks like an ear-plug that you can smash in your fingers, pack, manipulate and reshape, which can be packed into a socket and serves not only as a replacement to the bony particulate but also to the membrane. I thought it sounded
too good to be true until I tried it.

Look at this case:
As you can see, 13 is a goner. So I pulled it.

13 was partially in the patient’s smile line so he was very eager to get an implant as soon as possible. For some strange reason, he hated his flipper. Shocking! The problem was that he
had already lost bone because of the vertical root fracture. There was no way that I could tell
that patient, with confidence, that the edentulous area around 13 would be ready for an implant
in only six months without the use of some kind of socket preservation.
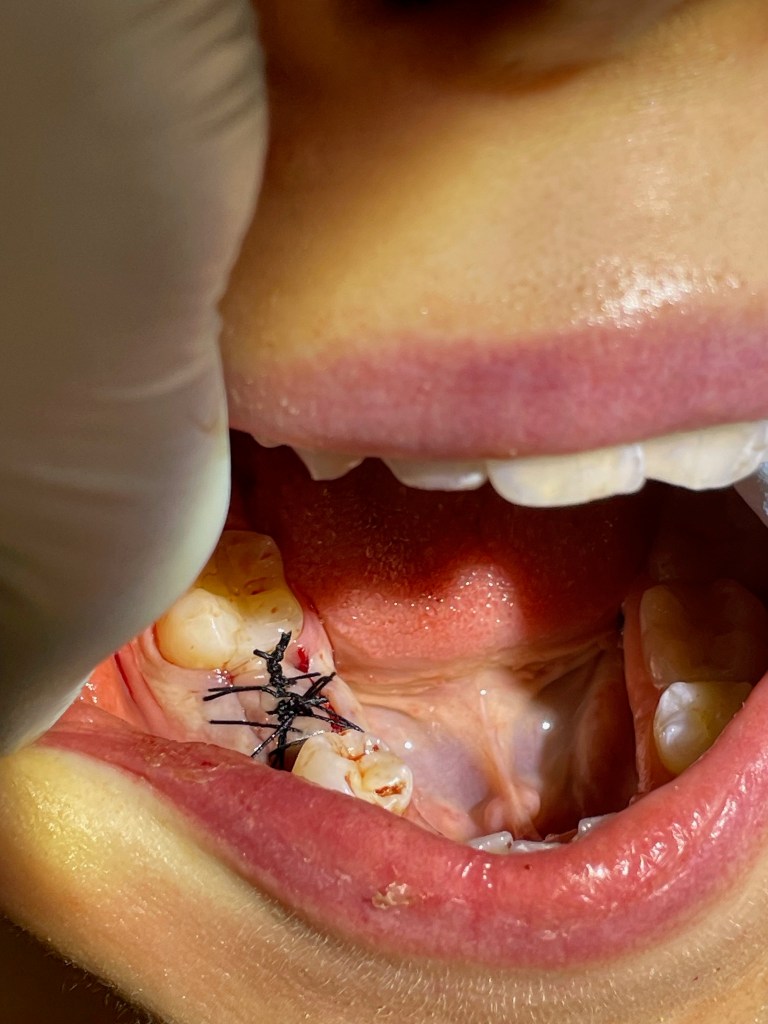
So I took a plug. This was an Osteogen plug from Impladent. In a matter of a few minutes, I
removed the plug from the packaging, packed it into the socket, and aggressively stitched it up.
This was socket preservation, but nothing like anything I had done before. No particulate, no membrane, no needles in the arm. Definitely no hip harvesting. It was, in essence, an earplug.
A bloody earplug that needed stitches, but still an earplug.

Here is how it looked 6 months later. Implant time.

Sadly, not all bony plugs are created equal. There are several plugs that exist in today’s
market, and they all look kind of similar. I’ll be at the FDC on June 21 in Orlando to sort it all
out. I hope you can join me.
Dr. Gupta will present the course “Demineralized and Cortico-What? A General Dentist’s Guide to the Most Uncomplicated and Predictable Bone Grafting Techniques Including Socket Preservation Without a Membrane” on Saturday, June 21 from 9 to 11 AM at the Florida Dental Convention. This course is free for FDA member dentists. Learn more and register at www.floridadentalconvention.com.
Biography
Ankur A Gupta, DDS, after completing a one-year GPR in Cleveland, started a practice from
scratch in 2005. Armed with what he considered adequate dental knowledge, hand skills, and a
personable demeanor, he watched as his practice floundered, finances became unpredictable,
and his lower back and spirit toward his profession became worrisome. Rather than continue
the trend, he made a guinea pig out of his office, family, and self, attempting any and all
personal and professional “experiments” in self-improvement.
More than a decade later, he enjoys an excellent practice, a solution oriented dental team; and
most importantly, a meaningful and positive identity. He happily shares the failures and
successes with dental and community groups throughout the country, always ending his
presentations with practical, implementable, step-by-step ways to be better.
Dr. Gupta graduated from the University of Michigan School of Dentistry in 2004. In 2005, after
completing a one-year General Practice Residency in Cleveland, Ohio, he and his partner Dr.
Nisha Gupta started North Ridgeville Family Dentistry. In addition to founding North Ridgeville
Family Dentistry, Dr. Gupta is a member of the American Dental Association, Greater Cleveland
Dental Society, Ohio Dental Association, ADA Success Speaker Corp and an active board
member and a speaker for Catapult Education’s Speaker Bureau.
Dr. Gupta is an AGD/PACE certified provider.
